This Technique Tuesday, our co-founder and equine veterinary surgeon, Jennifer Corley, is sharing her expertise on the Guttural Pouch Endoscopy technique. Have questions or comments? Drop them in the comment form below, and Jennifer will be more than happy to help! Stay tuned for more exciting insights and techniques.



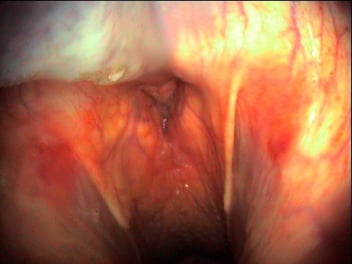
Examination of the guttural pouch using endoscopy allows for the identification of accumulated exudates, retropharyngeal abscessation, mycotic plaques, temperohyoid osteopathy or other abnormalities, as well as allowing for the collection of samples for cytology and culture and facilitating drainage of accumulated exudate.
View the Guttural Pouch Endoscopy video
Equipment Required:
• Endoscope (at least 1m long/maximum outer diameter of up to 12mm outer diameter)
• Good quality endoscopic light source
• Endoscopic biopsy forceps (at least 10-20cm/4-8 inches longer than the scope)
• Twitch (optional)
• Sedation (optional)
• K-Y jelly (optional)
• Equipment to take samples if required (aspiration tube, syringe, saline, culture bottles)
Procedure:
Placing an endocope in the guttural pouch is not a specialist technique, but it is difficult to perform consistently. Ideally this is carried out with good assistance. One person to restrain the horse, one to pass the scope and one to ‘drive’ the endoscope. Sedation should can be used but not until the function of the larynx or pharynx has been assessed. All of the equipment required for procedure should be prepared and to hand before passing the scope. If the horse cannot be restrained in stocks it is important to position the equipment so it can be rapidly moved away from the patient. Care must be taken to avoid being hit by the horses head or front legs. The simplest way to introduce the endoscope into the guttural pouch is to utilise the endoscopic biopsy forceps. The biopsy forceps will act as a stylet to allow the endoscope to be passed into the auditory canal and the guttural pouch. It is helpful if the person passing and the person driving the endoscope are both able to see the screen to coordinate the procedure. This technique is often carried out in animals with strangles and it can be performed with a direct endoscope single handed if necessary but obviously this is harder to do.
Technique:
1. Insert the biopsy forceps into the biopsy channel of the endoscope prior to inserting the endoscope into the nasal passages of the patient. Ensure that the forceps can pass through the channel easily and will extend 10-20cm past the end of the scope. Then withdraw the biopsy forceps and prepare to insert the endoscope into the nasal passage on the same side as the pouch to be examined.
2. Lightly lubricate the endoscope distally with a sterile water-soluble gel. The person passing the scope should lift the horse’s nostril with their non-dominant hand. Lightly resting this hand on the muzzle, use the thumb to push the endoscope ventrally and medially as it is passed into the nose with the other hand. It is important that the scope is passed via the ventral nasal meatus to avoid trauma to the ethmoturbinates. Pass the scope into the nasopharynx.
3. Once the scope is in the pharynx check both guttural pouch openings for discharge or swellings, observe the pharynx, epiglottis and arytenoids cartilages. Squirt a little water through the scope or lightly touch the pharynx with the scope so that swallowing may be observed.
4. To assess the function of the larynx briefly occlude both nostrils by pinching the muzzle causing the horse to breath in deeply. As this occurs the arytenoids should be pulled back with maximum abduction.
5. Upon visualisation of the salpingopharyngeal fold (the flap that covers the opening to the guttural pouch) extend the biopsy forceps (ensuring that they remain closed) and pass them lateral to the top corner of the fold and 2-3 cm into the auditory canal.
IT IS VERY IMPORTANT TO PLACE THE GUIDE IN THE TOP CORNER OF THE FOLD FOR SUCCESS.
6. After placing the biopsy forceps rotate the endoscope body to the left (right guttural pouch) or the right (left guttural pouch), which will cause the biopsy forceps to raise the fold, allowing the endoscope to be advanced into the auditory canal. As the endoscope enters into the guttural pouch, the biopsy forceps should be quickly withdrawn into the endoscope. The entire guttural pouch may then be examined.
7. To examine the contralateral guttural pouch it is typically easiest to completely withdraw the endoscope and place it in the nasal passages on the same side of the horse as the guttural pouch to be examined, although with practice both guttural pouches can sometimes be entered without repositioning the endoscope. Following repositioning of the endoscope the procedure is then repeated, remembering to rotate the endoscope in the opposite direction from that used on the first side. An alternative approach involves the use of a Chambers catheter or a plastic uterine infusion pipette bent approximately 20 degrees at a point 15 cm from the distal end of the catheter. The catheter is passed through the nasal passages contralateral to the guttural pouch of interest, with the endoscope in place in the ipsilateral nares. Under endoscopic visualisation the catheter is introduced into the pharyngeal opening of the guttural pouch, which will allow the endoscope to be passed lateral to the catheter into the guttural pouch.
8. Guttural pouch endoscopy should always be performed with caution, especially in the patient with a history of epistaxis, as this procedure may result in the destabilisation of an existing clot within the guttural pouch, resulting in resumption of haemorrhage. In this subset of patients one should be prepared for immediate surgical intervention prior to performing endoscopy. It is also important to remember the guttural pouch is a common site for respiratory infection to be carried and deep cleaning/sterilisation of the equipment will be necessary after the guttural pouch has been examined.
Further Resources:
View the Guttural Pouch Endoscopy video
EquiTrace Biosecurity whitepaper.
Link for further techniques here.
Equine Techniques App
https://apps.apple.com/us/app/equine-techniques/id451533346
References:
1. Burns J. Endoscopic instrumentation. In: Atlas of veterinary endosurgery Ed. Slovis NM, Mosby, St Louis, 2003, pp 3-27
2. Holcombe SJ, Jackson C, Gerber V, et al: Stabling is associated with airway inflammation in young Arabian horses. Equine Vet J 33:244-249, 2001
3. Hardy J, Leveile R. Diseases of the guttural pouches. Vet Clin North Am Equine Pract 19:123-158 2003
4. Harold McKenzie Endoscopy of the guttural pouch in The Equine Hospital Manual, Blackwell 2008